


Overview
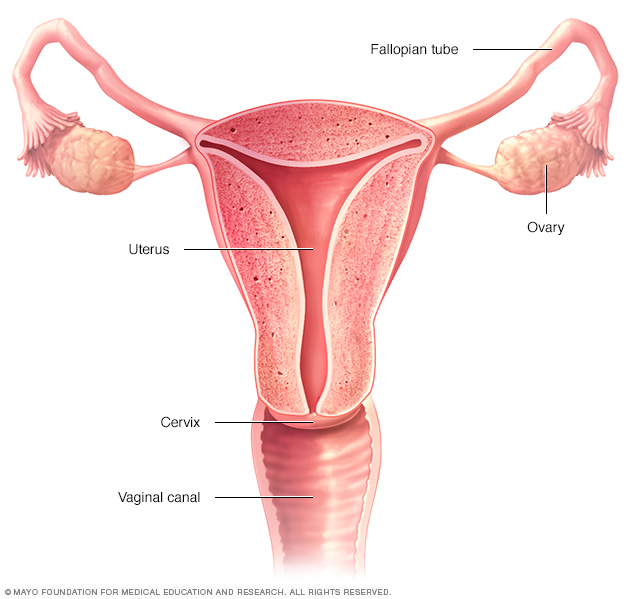
Ovarian cysts are sacs, usually filled with fluid, in an ovary or on its surface. Females have two ovaries. One ovary is located on each side of the uterus.
Each ovary is about the size and shape of an almond. Eggs develop and mature in the ovaries. Eggs are released in monthly cycles during the childbearing years.
Ovarian cysts are common. Most of the time, you have little or no discomfort, and the cysts are harmless. Most cysts go away without treatment within a few months.
But sometimes ovarian cysts can become twisted or burst open (rupture). This can cause serious symptoms. To protect your health, get regular pelvic exams and know the symptoms that can signal what might be a serious problem.
Symptoms
Most ovarian cysts cause no symptoms and go away on their own. But a large ovarian cyst can cause:
- Pelvic pain that may come and go. You may feel a dull ache or a sharp pain in the area below your bellybutton toward one side.
- Fullness, pressure or heaviness in your belly (abdomen).
- Bloating.
When to see a doctor
Get immediate medical help if you have:
- Sudden, severe abdominal or pelvic pain.
- Pain with fever or vomiting.
- Signs of shock. These include cold, clammy skin; rapid breathing; and lightheadedness or weakness.
Causes
Most ovarian cysts form as a result of your menstrual cycle. These are called functional cysts. Other types of cysts are much less common.
Functional cysts
Your ovaries grow small cysts called follicles each month. Follicles produce the hormones estrogen and progesterone and break open to release an egg when you ovulate.
A monthly follicle that keeps growing is known as a functional cyst. There are two types of functional cysts:
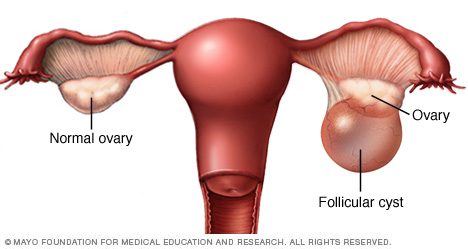
- Follicular cyst. About halfway through your menstrual cycle, an egg bursts out of its follicle. The egg then travels down a fallopian tube. A follicular cyst begins when the follicle doesn't rupture. It doesn't release its egg and continues to grow.
- Corpus luteum cyst. After a follicle releases its egg, it shrinks and begins producing estrogen and progesterone. These hormones are needed for conception. The follicle is now called the corpus luteum. Sometimes, the opening where the egg came from gets blocked. Fluid builds up inside the corpus luteum, causing a cyst.
Functional cysts are usually harmless. They rarely cause pain and often disappear on their own within 2 to 3 menstrual cycles.
Other cysts
There are other types of cysts that are not related to menstrual cycles:
- Dermoid cyst. Also called a teratoma, this cyst forms from reproductive cells that make eggs in the ovary (germ cells). The cyst can contain tissue, such as hair, skin or teeth. This type of cyst is rarely cancer.
- Cystadenoma. This type of cyst develops from cells on the surface of an ovary. The cyst might be filled with a watery or mucous material. A cystadenoma can grow very large.
- Endometrioma. Endometriosis is a condition that causes cells similar to those that line the inside of the uterus to grow outside the uterus. Some of the tissue can attach to the ovary and form a cyst. This is called an endometrioma.
Dermoid cysts and cystadenomas can become large and move the ovary out of position. This increases the chance of painful twisting of the ovary, called ovarian torsion. Ovarian torsion may reduce or stop blood flow to the ovary.
Risk factors
The risk of having an ovarian cyst is higher with:
- Hormonal problems. These include taking a fertility drug that causes you to ovulate, for example clomiphene or letrozole (Femara).
- Pregnancy. Sometimes, the follicle that forms when you ovulate stays on your ovary throughout pregnancy. It can sometimes grow larger.
- Endometriosis. Some of the tissue can attach to your ovary and form a cyst.
- Severe pelvic infection. If the infection spreads to the ovaries, it can cause cysts.
- Previous ovarian cysts. If you've had one ovarian cyst, you're likely to develop more.
Complications
They don't happen often, but complications can occur with ovarian cysts. These include:
- Ovarian torsion. Cysts that become large can cause the ovary to move. This increases the chance of painful twisting of the ovary (ovarian torsion). If this happens, you might have sudden, severe pelvic pain and nausea and vomiting. Ovarian torsion can also reduce or stop blood flow to the ovary.
- Cyst rupture. A cyst that bursts open (ruptures) can cause severe pain and bleeding inside the pelvis. The larger the cyst, the greater the risk of rupture. Vigorous activity that affects the pelvis, such as vaginal sex, also increases the risk of rupture.
Prevention
There's no way to prevent most ovarian cysts. But, regular pelvic exams help ensure that changes in your ovaries are diagnosed as early as possible. Be alert to changes in your monthly cycle. Make a note of unusual menstrual symptoms, especially ones that go on for more than a few cycles. Talk to your health care provider about changes that concern you.
Diagnosis
A cyst on your ovary can be found during a pelvic exam or on an imaging test, such as a pelvic ultrasound. Depending on the size of the cyst and whether it's filled with fluid or solid, your health care provider likely will recommend tests to determine its type and whether you need treatment.
Possible tests include:
- Pregnancy test. A positive test might suggest an early pregnancy. Corpus luteum cysts are normal to see during pregnancy.
- Pelvic ultrasound. A wandlike device (transducer) sends and receives high-frequency sound waves to create an image of your uterus and ovaries on a video screen (ultrasound). The image is used to confirm that you have a cyst, see its location, and determine whether it's solid or filled with fluid.
- Laparoscopy. A slim, lighted instrument (laparoscope) is inserted into your abdomen through a small cut (incision). Using the laparoscope, your provider can see your ovaries and any cyst. If a cyst is found, treatment is usually done during the same procedure. This is a surgical procedure that requires anesthesia.
- Tumor marker tests. Blood levels of a protein called a cancer antigen often are elevated in ovarian cancer. If your cyst appears solid and you're at high risk of ovarian cancer, your provider might order a cancer antigen 125 (CA 125) test or other blood tests. CA 125 levels can also be elevated in noncancerous conditions, such as endometriosis and pelvic inflammatory disease.
Sometimes, less common types of cysts develop that a health care provider finds during a pelvic exam. Solid ovarian cysts that develop after menopause might be cancerous (malignant). That's why it's important to have regular pelvic exams.
Treatment
Treatment depends on your age and the type and size of your cyst. It also depends on your symptoms. Your health care provider might suggest:
- Watchful waiting. In many cases you can wait and be reexamined to see if the cyst goes away after a few months. This is typically an option — regardless of your age — if you have no symptoms and an ultrasound shows you have a small, fluid-filled cyst. You may have several follow-up pelvic ultrasounds to see if your cyst changes in size or appearance.
- Medicine. Hormonal contraceptives, such as birth control pills, keep you from ovulating. This may keep you from getting more ovarian cysts. But, birth control pills won't shrink an existing cyst.
-
Surgery. Your provider might suggest removing a cyst that is large, doesn't look like a functional cyst, is growing or causes pain. Some cysts can be removed without removing the ovary (cystectomy). In some cases, the ovary with the cyst is removed (oophorectomy).
Surgery can often be done using minimally invasive surgery (laparoscopy) with a laparoscope and instruments inserted through small cuts in your abdomen. If the cyst is large or cancer is a concern, an open procedure using a larger cut may be needed.
An ovarian cyst that develops after menopause is sometimes cancer. In this case, you may need to see a gynecologic cancer specialist. You might need surgery to remove your uterus, cervix, fallopian tubes and ovaries. You may also need chemotherapy or radiation.
Preparing for an appointment
Your first visit may be with your primary care provider or a specialist in conditions that affect the female reproductive system (gynecologist).
Think about bringing a family member or friend with you to the appointment, if you can. They can listen to what your provider says and help you recall information later.
What you can do
Before your appointment, make a list of:
- Your symptoms, including those that seem unrelated to the reason for the appointment, and when they began
- All medicines, vitamins, herbs and other supplements you take and the dosages
- Your medical history, including menstrual irregularities
- Questions to ask your health care provider
Questions to ask include:
- What's likely causing my symptoms?
- What tests might I need?
- Will my cyst go away on its own, or will I need treatment?
- Do you have printed materials or brochures I can have? What websites do you recommend?
Don't hesitate to ask other questions as they occur to you during your appointment.
What to expect from your doctor
Questions your provider might ask include:
- How often do you have symptoms?
- How bad are your symptoms?
- Do your symptoms seem related to your menstrual cycle?
- Does anything make your symptoms better?
- Does anything make your symptoms worse?
- Have you had ovarian cysts in the past?
Your provider will ask other questions based on your responses, symptoms and needs. Being ready to answer the questions will help you make the most of your appointment time.
© 1998-2024 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use